Congenital Neck Masses
What is a congenital neck mass?
A congenital neck mass is a growth that is present at birth and slowly becomes noticeable to the patient or family. Although the neck abnormality is present since birth, the resulting lump may not appear until much later in life.
What are the types of congenital neck masses?
Congenital neck masses can take many forms. The most common congenital masses that are treated by an ear, nose, and throat specialist are:
- Branchial Cleft Anomalies (abnormalities)
- Thyroglossal duct remnants (like cysts)
- Lymphangiomas (cystic hygromas)
- Hemangiomas (blood vessel abnormalities)
- Dermoid cysts
Each of these causes will be discussed in detail below as well as Deep Neck Infections.
BRANCHIAL CLEFT ANOMALY
What are Branchial Cleft Anomalies?
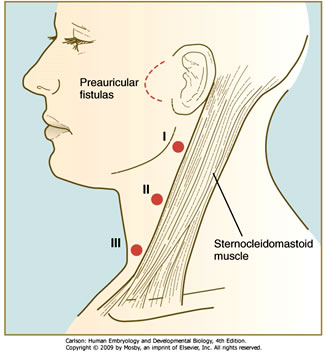
Branchial cleft fistulas (tracts) and cysts (called anomalies) are found in the neck and are composed of tissue trapped in the developing neck. These anomalies appear as a soft lump or draining opening on one side of the neck. They can appear in any age group yet are very common in the first decade of life. Because these anomalies develop in the growing embryo, any tract that forms in combination with a cyst follows a fairly predictable pattern. The tracts connect the cyst to the inside of the throat at a specific area. It is important to understand this relationship so that the entire tract can be excised and will not recur.
There are three kinds of branchial cleft anomalies. A first branchial cleft anomaly is more unusual and may be involved with the nerve that moves the facial muscles (Facial nerve).
If your child has been diagnosed with a branchial cleft anomaly, many times the physician will order a CT scan (cat scan). This test will allow us to identify the exact location of the mass and/or tract as well as its relation to blood vessels and nerves in the neck.
Once an anomaly has been identified, treatment consists of surgically removing the cyst before it has a chance to get infected and become an abscess. Surgery is performed under general anesthesia by making an incision over the cyst or draining area. Every effort is made to place the incision in an existing skin crease so that cosmetically the child’s scar will be minimal. Plastic surgery techniques are always used to close the incision. Branchial cleft anomalies are usually removed as an outpatient procedure. These operations usually last between one and two hours. Ear, nose and throat specialists have extensive training in surgery of the neck, making them the most qualified physicians for this type of surgery.
If the cyst has become infected (or formed an abscess) prior to removal, incision and drainage of the abscess may be necessary first, followed by treatment with antibiotics. The cyst and tract can then be safely removed at a later date.
THYROGLOSSAL DUCT REMNANTS
What are Thyroglossal Duct Cyst?
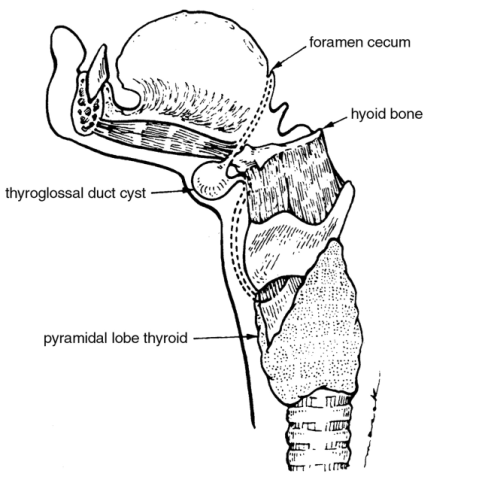
Thyroglossal duct cysts are cysts that are left over when the thyroid migrates from the base of the tongue into the neck before birth. The cyst is connected to the back of the tongue by a small tract. The cyst usually lies in the middle of the neck in front of the “Adam’s Apple”.
Thyroglossal duct cysts usually show up in the first ten years of life, but may be found in older children or even adults. It is a benign cyst that usually contains mucous or even pus-like fluid. Many times, these cysts will not be evident until your child has an upper respiratory infection (cold). After which, the cyst will suddenly appear in the front of the neck. The sudden appearance or rapid enlargement of these cysts can be alarming. If a cyst is infected, many times antibiotics and/or drainage may be necessary to control the infection prior to definitive removal.
However, if the cyst appears without infection, and you wish to avoid further problems with infection, surgical removal is best performed before the cyst is ever infected.
Thyroglossal duct cysts are usually in the middle of the neck and seem to move up and down during swallowing. Because thyroid tissue may be inside the cyst, it is important to make sure that the thyroid gland has developed normally (and that not all the thyroid tissue is within the cyst). Your doctor may order an ultrasound and/or a thyroid scan to make sure the “cyst” is not the only functioning thyroid gland.
Once these tests have been completed, excision of the cyst may be performed as an outpatient procedure. This operation usually takes 45 minutes to an hour. Your child may leave the same day but will require decreased activity in the first week after surgery.
LYMPHATIC DRAINAGE ABNORMALITIES(CYSTIC HYGROMAS)
What is a lymphangioma?
A lymphangioma is the result of an abnormal collection of lymph channels in the body. These channels usually link the disease-fighting lymph nodes together. During fetal development connections may occur causing cysts made up of these channels to grow. Large extensive collections of these are known as lymphangiomas or cystic hygromas. They grow steadily with the child and usually surround normal muscles, blood vessels, and nerves. These cysts can involve the neck, oral cavity, face and airway. They can also extend into the chest.
How are lymphangiomas recognized?
Because of their size, lymphangiomas are usually visible as a large compressible (can flatten when pushed on) mass. Those not noticed at birth are recognized before most children reach their second birthday.
Why are lymphangiomas of concern?
Lymphangiomas grow around normal muscles, blood vessels, and nerves. They may become quite extensive and cause significant cosmetic (appearance) deformities and functional disabilities. They may prevent the child from swallowing normally, speaking, or even breathing. The cysts are not cancerous. However, they continue to grow and many times cannot be completely removed without sacrificing an important normal structure.
How is a lymphangioma diagnosed and treated?
DIAGNOSIS: These lesions are first evaluated by physical examination. Magnetic Resonance imaging (MRI) is the imaging study that gives the best information regarding the extent and location of the cystic hygroma. X-rays and CT scans may also be used to help fully realize the extent of the cyst.
Once the location and extent into surrounding structures has been studied, therapy best suited for the patient can be initiated.
TREATMENT: There are generally two methods used to treat lymphangiomas:
Medical – This method utilizes medications (sclerosing agents) injected into the cyst to reduce the size of the cyst. This means that the cyst is not removed, but “scars” down on itself so that growth stops.
Surgical – This approach to treatment of a lymphangioma is excision of the cyst with a surgical procedure. *If airway involvement is present, the lymphangioma is removed as soon as it is diagnosed. Sometimes, a TRACHEOTOMY may be needed to secure the airway.
Our practice’s philosophy is to surgically remove those lesions that appear to be removable with a single operation. Many times this is done in the first few months of life. If, however, the lesion is quite extensive and places the child at risk for nerve, blood vessel, or muscle damage, or, would result in significant deformity in the appearance of the child, sclerosing agents are recommended.
HEMANGIOMA
What is a hemangioma?
A hemangioma is an abnormal growth of blood vessels that are formed before or shortly after birth. They can be very small (pinpoint) or grow to be quite large. They need to be distinguished from vascular malformations (abnormal connections between blood vessels) because treatment is different.
What do hemangiomas look like?
Hemangiomas may look like small red pimples on the skin, large bulging bluish-red masses protruding from the forehead or eyelid, or soft compressible bluish masses in the neck. Hemangiomas may also involve the breathing tube just below the voice box (subglottic area) causing noticeable breathing problems.
Hemangiomas usually start to grow larger shortly after birth (proliferative stage) reaching a peak at 18 months to 2 years of age. At that point, most hemangiomas will start to shrink (involute). This process may take several years.
How are hemangiomas diagnosed and treated?
DIAGNOSIS: Magnetic resonance imaging (MRI) is used to diagnose hemangiomas. Sometimes, a biopsy (a small amount of tissue from the lesion) is required to confirm the diagnosis.
TREATMENT: If hemangiomas are located in areas that cause the patient breathing problems (in the airway) or problems seeing (covers part of the eye), steroids may be given to shrink the mass. However, steroids only give temporary relief and therefore need to be given over long periods of time. In addition, this form of treatment has its own risks due to side effects of steroids. Should this treatment option be recommended, your physician will discuss these issues in detail with you.
If steroids are not advised, then surgical therapy is an alternative to remove or reduce the size of the hemangioma more permanently. Surgical therapy using laser has been very helpful in shrinking or excising (removing) hemangiomas.
Both the CO2 (carbon dioxide) and YAG laser are used in our practice.
DERMOID CYST
What is a dermoid cyst?
A dermoid cyst is a mass containing skin, hair, and skin glands that are trapped under the skin, usually located in a line drawn from the middle of the forehead to the bottom of the neck. An ear, nose, and throat specialist is commonly consulted to evaluate a congenital dermoid cyst located on the scalp, face, in the nose or on the neck.
How is a congenital dermoid cyst recognized?
A dermoid cyst is recognized as a small, painless swelling on the face, scalp, nose, or neck. They can range in size from 1 to 4 centimeters (about 1/2 to 3 inches) across. These cysts may need to be differentiated from other congenital neck masses, which can be done with careful physical exam. Sometimes, imaging (picture type) studies such as CT scans or MRI’s are needed. CT scans are also useful to look for any part of the dermoid cyst that may extend into the skull bone. This is especially true of nasal dermoid cysts, which look like a small hole on top of the nose, usually with a hair sticking out.
How are dermoid cysts treated?
Dermoid cysts need to be surgically removed and this is usually a simple surgical procedure. Nasal dermoid cysts, however, require more extensive evaluation looking for invasion into the skull, and may require surgical removal by an ear, nose, and throat surgeon, working with a neurosurgeon.
DEEP NECK INFECTIONS
What is a “deep neck” infection?
A “deep neck” infection refers to an infection or abscess (collection of pus) located deep under the skin near blood vessels, nerves, and muscles.
Where is the “deep neck” located?
There is a band of tissue in the neck called the cervical fascia, which divides the neck into superficial (just under the skin) and deep layers. The deep layer of the neck is then further subdivided into various spaces. A deep neck infection is an infection that is located in one of these spaces in the deep layer of the neck. Ear, Nose, and Throat surgeons are experts in the anatomy of the neck including these spaces.
Although a deep neck infection can be seen in any of the deep neck spaces, the most common spaces in which deep neck infections are found in children are:
- RETROPHARYNGEAL SPACE
This space is located directly behind the mouth.
The lymph nodes (infection fighting structures) that drain the ADENOIDS, SINUSES, nose, and pharynx (back of throat) are located in this space. Infections in any of these areas can result in spread of infection to these lymph nodes, resulting in lymphadenitis (infection of the lymph nodes) and abscess formation (collection of pus). The retropharyngeal lymph nodes become significantly smaller after five years of age; therefore, this infection is usually seen only in younger children. - PERITONSILLAR SPACE
Located in the tissue around the tonsil in the back of the throat.
Infection in this space usually results from an untreated infection of the tonsils (TONSILLITIS). This type of infection is known as a peritonsillar abscess or quinsy (a collection of pus in the peritonsillar space) and is probably the most common type of deep neck infection. This infection can occur at any age. - PARAPHARYNGEAL SPACE
It is located just behind the carotid artery (delivers blood to the head), just to the side of the throat. Infections in this area are due to common upper respiratory infections that spread to the lymph nodes located in this space. If an infection in this area remains untreated, the neck swells and the child stops moving the neck, indicating pain. - SUBMANDIBULAR SPACE
This space is located under the jaw on each side. Infection in this space is usually the result of a dental infection and is known as Ludwig’s angina. It is more commonly seen in adolescents, but can also occur in younger children.
What causes a deep neck infection?
In children, deep neck space infections are usually caused by more common infections, such as dental abscesses, tonsillitis, or respiratory infections that are located “above” these spaces that spread into these deep spaces by the lymphatic system (system that drains fluid in the body).
Lymph nodes (contain disease fighting cells) in these spaces then become infected (lymphadenitis).
Additionally, bacteria can be directly introduced to a deep neck space by trauma affecting the area (more commonly seen in adults).
Finally, an infection from one deep space may spread to another deep space directly.
What are the symptoms of a deep neck infection?
Some of the more common symptoms of a deep neck infection include: Decreased ability to move the neck, asymmetry of the neck and back of the throat, difficulty or pain when swallowing, drooling, sick appearance, fever, and swelling in the neck, under the jaw, or on the face. Difficult or fast breathing may also be noted if airway involvement has occurred.
What are the complications of a deep neck infection?
The complications of deep neck infections can be life threatening; therefore, early detection and treatment are of extreme importance.
Some of these complications include:
- Airway obstruction -probably the most serious initial complication; a deep neck infection can create swelling that pushes in on the airway causing partial or complete obstruction (blockage)
- Spread of the infection – deep neck infections can spread to other deep neck spaces, as well as the mediastinum (middle chest cavity), lungs (empyema-pus in the lungs), bloodstream (sepsis), and bones (osteomyelitis)
- Thrombus (clot) formation in arteries and veins of the neck
- Nerve involvement – the nerves which affect vocal cord movement, eyelid closure, sweating, and pupil constriction may also be pressed upon causing nerve dysfunction
How is a deep neck infection evaluated?
Because the infection is only noted by swelling in the neck a careful history and physical examination is important when suspecting a deep neck infection.
Blood tests useful in the evaluation of a deep neck infection include blood counts (for signs of infection), chemistry profiles (to check for lack of fluid intake), and blood cultures (to check if the infection has spread to the blood).
X-rays of the neck, teeth, and chest may also be indicated depending on the type of deep neck infection suspected.
CT scans are the standard of care (test of choice) when evaluating the extent of a deep neck space infection. They give very accurate pictures of the infection’s location, which is especially useful if surgical drainage of the infection is required.
How is a deep neck infection treated?
Because of the immediate threat of airway obstruction, most deep neck infections require hospitalization. When the airway is narrowed, an endotracheal (breathing tube passed through the mouth) or nasotracheal (breathing tube passed through the nose) tube may be placed to hold open the airway until the infection can be treated. In severe cases, when a breathing tube cannot be inserted, a TRACHEOTOMY may be temporarily required.
Most patients will have a history of decreased fluid and food intake, therefore fluids given by vein will usually be required.
All patients with deep neck infections are started on antibiotics given by vein. In a select group of patients, careful hospital observation and antibiotics may be enough to treat the infection. However, surgical drainage is required in some cases. Please see DRAINAGE OF NECK ABSCESSES for details.
When is an ear, nose, and throat specialist involved in the treatment of a deep neck abscess?
Because airway obstruction is always a concern with a deep neck infection, an ear, nose and throat specialist is usually consulted immediately to help manage the airway and determine whether surgical therapy is needed.
